Challenging Case of Parotitis: A Comprehensive Approach
Theoretical Parotitis
The conclusion and the executives of parotitis can be testing. Patients frequently present with torment and edema in the neck, jaw, head, and ear because of blockage of the organ. Parotitis is normally brought about by a contamination inside the parotid organ and encompassing lymph hubs, and the disease can spread to neighboring cervical fascial planes and cause significant difficulties if not oversaw effectively. Explicit rules for the short term the executives of parotitis are restricted, and short term treatment disappointments are normal, requiring ongoing treatment with different expansive range anti-microbials. In the current case, a far reaching patient-focused methodology was utilized to treat a lady whose covering clinical conditions, way of life, and work factors prompted a disease of the parotid organ.
Testing instances of parotitis require an all encompassing way to deal with patient consideration, which considers the entire individual instead of the illness in segregation. Albeit parotid organ diseases are phenomenal, cases in the writing have been archived since the 1800s.
Parotid organ brokenness is more normal in patients who are at limits old enough, in patients postoperatively, or in patients who are immunocompromised. Parotitis is named suppurative or nonsuppurative. The suppurative sort is brought about by polymicrobial microbes that climb from the oral cavity, dominatingly Staphylococcus species. The nonsuppurative causes are various and incorporate viral, immune system, and metabolic causes. Embroiled viral microorganisms incorporate mumps, Epstein-Barr infection, flu, coxsackievirus, and cytomegalovirus.
Other contributing conditions incorporate immune system processes, cystic fibrosis, lack of hydration, diabetes, liquor abuse, sarcoidosis, sialolithiasis, and harmless or dangerous tumors.3 Complications of parotitis might include expansion of contamination into touchy constructions of the neck, prompting enormous enlarging, obstructive respiratory dysfunctions, septicemia, facial bone osteomyelitis, and septic jugular thrombophlebitis
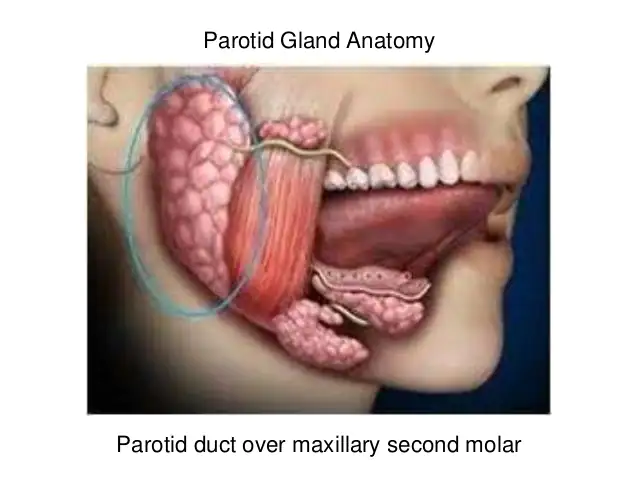
Treatment for patients with parotitis starts safely and turns out to be more intrusive if introductory medicines fail.2 The backbone of short term treatment incorporates anti-microbials, satisfactory hydration, great oral cleanliness, privately applied hotness, and aversion of anticholinergic medications.Initial anti-microbial routine starts with antistaphylococcal penicillin for 10 to 14 days. Antibiotics that target Staphylococcus, anaerobes, and gram-positive creatures ought to be considered as a result of the closeness of the oral pit to the Stensen conduit, which channels salivation from the parotid organ into the mouth.
Notwithstanding conventional anti-infection treatment, parotid organ back rub, sialogogues, and osteopathic manipulative treatment (OMT) may assume an adjunctive part by further developing parotid organ blockage, working with conveyance of drugs to the site of contamination, and easing pain. Management procedures that think about illness microbes, touchy physical constructions, parotid organ mechanics, and a patient’s interesting contributing danger factors give a comprehensive methodology.
This report features a thorough way to deal with a difficult instance of parotitis that was muddled by the patient’s danger factors.
Report of Case
A 50-year-elderly person introduced to the family medication center with left-sided preauricular agony and expanding that emanated into her neck and jaw. The aggravation started fourteen days sooner and was deteriorating; on show the patient appraised it 9 on a 10-point scale, with 10 being the best aggravation. Of note, she was seen 2 weeks beforehand at a dire consideration office, and 2 unique courses of anti-infection agents (cephalexin and amoxicillin clavulanate) were endorsed. These meds offered no alleviation.
Extra objections included dysphagia, cervicalgia, and xerostomia. Her clinical history included overactive bladder, nervousness, a sleeping disorder, ongoing hyponatremia, and low body weight. Her meds included 5 mg of oxybutynin every day, 200 mg of sertraline hydrochloride day by day, and 100 mg of trazodone hydrochloride at sleep time. She had a 50-pack/y history of tobacco use and long-standing history of liquor abuse. In her day by day work as a phone administrator at a call community, she wore a cozily fitting headset that compacted the whole left half of her face.
Her important bodily functions were typical except for a low weight file of 18. She showed up sick, underweight, and restless. There was delicacy to palpation at the left mastoid interaction and momentous left-sided enlarging foremost and second rate compared to the outside hear-able waterway. Passed on front cervical lymphadenopathy back to the jaw point estimated 3.5 cm. Outer muscle assessment discoveries remembered diminished cervical scope of movement for left sidebending; occipitoatlantal sidebent left, pivoted right; atlantoaxial turned right; C2 flexed, pivoted right, sidebent right; C3 expanded right, sidebent right; front C1 left; back C2 left; back C3 left; back C2 right; back C5 right; and myofascial limitation in the neck. Cranial dysfunctions incorporated a left cranial twist, left sidebending turn, and an inside pivoted and stationary left transient bone. The rest of the actual assessment discoveries were unexceptional.
At the underlying visit, 500 mg of ceftriaxone was given intramuscularly, and earnest head figured tomography (CT) was requested. The CT picture showed diffuse parenchymal upgrade in the left parotid organ (Figure) and related intense cervical lymphadenopathy. Working findings included intense suppurative parotitis versus nonsuppurative parotitis brought about by the antagonistic impacts of her anticholinergic drug (eg, xerostomia) and further muddled by parotid organ check because of the headset she wore working. Her different judgments included physical dysfunctions of the skull and neck, local cervical lymphadenitis, leukocytosis, and uneasiness.
After analytic imaging uncovered parotitis, a 10-day course of levofloxacin was recommended. The specific serotonin reuptake inhibitor and trazodone dosages were diminished to limit xerostomia and hyponatremia. She was additionally urged to keep a sound weight, quit smoking, and utilize a noncompressing headset at work. Different modalities included warm packs, sialogogues, and at-home back rub of the parotid organ.
Moreover, OMT was applied at 5 meetings more than 2 months, zeroing in on cranial, lymphatic, and delicate tissue substantial dysfunctions. Arrangements were booked around at regular intervals. Explicit procedures included cranial adjusting, suboccipital discharge, cervical Still strategy, cervicothoracic myofascial discharge, cervical and periauricular lymphatic seepage, and strain-counterstrain.7-10 It is hard to measure the impacts of OMT in light of the fact that the anti-microbials and anticholinergic drugs were changed simultaneously. Notwithstanding, she emotionally detailed further developed agony and diminished neck expanding after the primary OMT meeting. After the second OMT meeting, she detailed goal of agony, and the lymph hub was as of now not obvious. Despite the fact that she had total goal of these side effects by the 2-month follow-up, she kept on encountering prescription actuated xerostomia. Furthermore, Clostridium difficile colitis created, which settled throughout the following month with fitting administration.
Conversation
The parotid organ creates and conveys salivation into the oral cavity.11 These emissions help to soak food boluses, secure oral mucosa and teeth, and forestall rising of microbes into the gland.11 The parotid organ is precisely animated by encompassing designs (muscles, belt, and bone) during rumination and controlled by parasympathetic control. Dysfunction of the organ can prompt parotitis.
Ongoing xerostomia can incline patients to parotitis on the grounds that the absence of emissions considers climb of microscopic organisms into the organ from the oral cavity.3,5 The added substance anticholinergic impacts of this present patient’s drugs, including the long haul, high-portion particular serotonin reuptake inhibitor, trazodone, and oxybutynin, probable prompted overpowering xerostomia, accordingly inclining her to salivary balance and microbe ascension. Altering her meds ended up being trying, as diminishing the portion of her prescriptions expanded her uneasiness.
With regards to the mechanical activity of the parotid organ and the various physical dysfunctions recognized in this persistent, the compressive headset use was unsettling. These limitations might have assumed a part in diminishing microbe freedom from the organ or forestalling sufficient anti-infection conveyance to the impacted tissue. The belt of the human body is an exceptionally powerful construction. Belt gives a moveable conductor through which the neurovascular support for all organ frameworks flows. Even limited quantities of tension after some time can have an added substance impact, bringing about critical pathologic changes, as shown by our patient’s substantial dysfunctions.
The capacity of lymphatic therapies to further develop lymphatic balance has been portrayed in the osteopathic writing since the hour of Andrew Talor Still, MD, DO. Lymphatic balance brought about by outer muscle limitation has been accounted for to expand disease hazard, and diminishing the limitation can work on the condition.15 There are no reports in regards to the utility of OMT for parotitis, as far as anyone is concerned; in any case, a few examinations have archived fruitful utilization of lymphatic OMT as adjuvant treatment for other head and neck contaminations, for example, otitis media and center ear emissions in children.16 Steele et al16 carried out an OMT convention that included lymphatic procedures, for example, cervicothoracic myofascial discharge in patients with intense otitis media and radiation that brought about a quicker pace of recuperation than clinical administration alone.
Parotitis treatment rules frequently incorporate a fundamental parotid back rub, which plans to increment salivary stream. Contrasted and a fundamental back rub procedure applied to the parotid.
Conclusion
The foundation of the osteopathic approach relies on consideration of the whole person with respect to the surrounding clinical picture. In approaching this case, it was important to consider the unique patient characteristics and all facets of the disease. This approach included focusing on the total health of the patient by improving the mechanics of the involved structures with OMT, eliminating pathogens, optimizing medication choices, and decreasing patient risk factors.